Anterior cruciate ligament reconstruction has become one of the most commonly performed surgical procedures to the injured knee joint. The rationale for surgical treatment is to stabilize an unstable joint, or potentially unstable joint, with the aim of preventing giving way of the joint under load. Joint stabilisation has been shown to decrease meniscal and articular cartilage damage, which potentially decreases the incidence and severity of later osteoarthritic change. Surgical techniques have advanced greatly over the past decade with accelerated rehabilitation protocols now being developed and preferred.
Non surgical management of ACL tears has also been proven to be effective in particular cases. This involves a course of Physiotherapy to help the tendon heal and restore optimal muscle function. Here at Gold Coast Sport and Spinal are therapist are very experienced inthe management of bot surgical and non surgical ACL year Recovery.
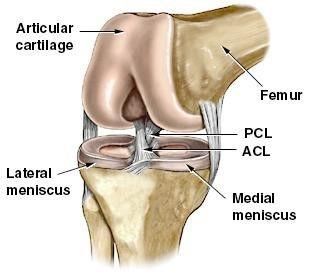
THE ANTERIOR CRUCIATE LIGAMENT
The Anterior Cruciate Ligament (ACL) is a short strong ligament composed of three main bundles of fibres located inside the knee. Simply described, it attaches from the front edge of the tibia and passes upwards, backwards, and outwards to attach to the inside of the outer condyle of the femur. The ACL controls excess movement of the tibia forwards on the femur during most movements of the knee. To tear, damage, or fully rupture the ACL, therefore usually involves a hyperextension or twisting of the knee with the foot on the ground eg. changing direction sharply when running.
SURGICAL REPAIR OF THE ACL
Once ruptured, the ACL can’t be rejoined effectively. The ligament must be ‘reconstructed’, usually with a graft from the hamstrings from the same leg. Sometimes the middle third of the patella tendon is used if extra stability is required. This procedure is done via an arthroscope (key hole surgery). During surgery, the ruptured ACL stumps are removed and meniscal (cartilage) surgery is carried out if required. The ACL is then reconstructed. This involves the surgeon harvesting the graft and skilfully positioning it inside the knee to replace the ACL. It is anchored in holes drilled in the Femur and Tibia usually by a combination of screws, buttons and sutures. The decision on selecting the type of graft is made by the Orthopaedic Surgeon and depends on the degree of instability and the requirements of the knee once rehabilitation is completed. It is precisely positioned to offer adequate tension to stabilize the knee and prevent forward movement of the Tibia on the Femur. During the early post-operative healing period exercise must be limited to avoid strain on the graft fixation sites, stretching of the graft (known as creep) and the sutures. The knee joint must also be allowed to settle after the trauma of surgery. The graft itself is strongest directly after implantation and is at its weakest at approximately the sixth week after surgery. At that time it continues to remodel and slowly regains strength. It can take up to a year to reach full maturity, but may never regain the full strength of the original natural ligament. A return to sport is usual at approximately 6-8 months after surgery.
LIGAMENT REPAIR FAILURE
This can occur due to:
- Inadequate muscular and proprioceptive rehabilitation
- Re-trauma
- Shock loading
- High level sporting activity
- Spontaneous rupture
Therefore, a thorough structured rehabilitation is of vital importance to the short and long term success of your reconstruction. It is important to note that strain to ACL reconstructions can be altered significantly by joint angle and the type of muscular force applied to the knee at that angle.
GENERAL PRINCIPLES FOR REHABILITATION
It is important to note that the following program outlines guidelines for rehabilitation after ACL reconstruction. Your physiotherapist will modify it at times to suit your individual requirements. All patients progress at different rates, have different requirements and goals and have differing levels of pathology (other ligament, menisci, joint surface damage).
- Be sensible in your approach to rehabilitation and do not overestimate your ability or progress. Before you attempt any new activity, discuss and clear it with your physiotherapist and surgeon.
- Exercises need to be done 3-5 times per day - little and often is better than an extensive overload period.
- Pain, heat and increasing swelling in the knee are bad: Any of these symptoms can mean that you may be overdoing your exercises. After major knee surgery your knee will be sore. It is important to understand that discomfort is normal particularly when performing some of the stretching exercises. In addition, your knee may ache after an exercise session. This is expected and normal so long as it is not associated with any significant increase in swelling. 'Bad' pain is usually sharp and severe in nature. Activities causing such a problem should be stopped and advice sought from your physiotherapist.